Cisplatin Increases Serum Creatinine, Serum Cystatin c and Urinary NGAL in Cervical Cancer IIB at Dr. Soetomo Hospital, Surabaya
Tanggal : 01 Nov 2016 10:13 Wib
Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Airlangga
Jl. Mayjen Prof dr Moestopo 6-8, Surabaya 60131, Indonesia
Email: rozi_nana@yahoo.co.id
Telephone: +6285277117500
Brahmana Askandar
Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Airlangga
Jl. Mayjen Prof dr Moestopo 6-8, Surabaya 60131, Indonesia
Mochammad Thaha
Department of Internal Medicine, Faculty of Medicine, Universitas Airlangga
Jl. Mayjen Prof dr Moestopo 6-8, Surabaya 60131, Indonesia
Keywords: cervical cancer IIB, neoadjuvant cisplatin, serum creatinine, serum cystatin C, urinary Neutrophil Gelatinase-Associated lipocalin.
Word count: 3766
ABSTRAK
Tujuan: Penelitian ini bertujuan menilai peningkatan parameter ginjal berupa serum kreatinin, cystatin c serum dan NGAL urine setelah Cisplatin ke-4.
Metode: Penelitian ini merupakan analitik observasional dengan time series design. Dilakukan pada 14 pasien kanker serviks IIB yang memenuhi kriteria inklusi dan ekslusi. Dilakukan pemeriksaan serum kreatinin, cystatin c serum dan NGAL urine sebelum dan 12 jam setelah Cisplatin 1 s.d ke-4.
Hasil: Pada hasil penelitian, dari 14 sampel penelitian didapatkan perbedaan signifikan peningkatan (p<0.05) kreatinin serum sesudah Cisplatin ke-2 dan ke 4, perbedaan signifikan peningkatan (p<0.05) cystatin c serum sesudah Cisplatin ke-4 dan terdapat peningkatan NGAL setelah cisplatin 1 namun tidak signifikan. NGAL urine meningkat pertama kalinya dibandingkan kreatinin serum dan cystatin c serum.
Simpulan: Terdapat peningkatan kreatinin serum, cystatin c serum dan NGAL urine. NGAL urine meningkat pertama kalinya, sehingga NGAL urine dapat dijadikan biomarker deteksi dini kerusakan ginjal dibandingkan kreatinin serum dan cystatin c serum setalah pemberian cisplatin pada kanker serviks IIB.
ABSTRACT
Aim: To compose increment of renal parameters : serum creatinine, serum cystatin C and urinary NGAL after 4th Cisplatin.
Methods: This was an observational analytic study paired with time series design. The study was conducted on 14 stage-IIB cervical cancer patients who met inclusion and exclusion criteria. We administered serum creatinine, serum cystatin C and urinary NGAL before and 12 hours after 1st to 4th Cisplatin.
Results: From 14 subjects sample, there was significant increase of serum creatinine (p <0.05) after 2nd and 4th Cisplatin, a significant increase of serum cystatin C (p <0.05) after 4th of Cisplatin and increased urinary NGAL, although not significant. However, urinary NGAL increased first, compared to serum creatinine and serum cystatin c.
Conclusion: Serum creatinine, serum cystatin c and urinary NGAL are increasing in cervical cancer IIB patients. Following cisplatin treatment on IIB cervical cancer, urinary NGAL increased first, earlier than serum creatinine and serum cystatin c, so urinary NGAL becomes a useful biomarker of AKI.
INTRODUCTION
According to data from WHO in 2013, the incidence of cancer increased from 12.7 million cases in 2008 to 14.1 million in 2012, while the number of deaths increased from 7.6 million people in 2008 to 8.2 million in 2012. Cancer was the number two cause of death in the world by 13% after cardiovascular disease. In Indonesia, the prevalence of cancer was also quite high. Based on data from Health Research (Riskesdas) in 2013, the prevalence of cancer in Indonesia was 1.4 per 1000 population, or about 330,000 people.1 At Dr. Soetomo Hospital, there were 506 new cases diagnosed as cervical cancer in 2013; 212 of them were stage IIB cervical cancer. Whereas in 2014, there was an increasing number of new cases of cervical cancer, as many as 842 patients, 196 patients of whom had stage IIB cervical cancer. Therapy protocol of IIB cervical cancer patients in Gynaecological Oncology Division of Dr. Soetomo Hospital is the administration of neoadjuvant chemotherapy with cisplatin 4 times (dose of 50 mg/kg/m2/week), followed with operability evaluation.2
Cisplatin (cis-diamminedichloroplatinum (II), CDDP) is an antineoplastic drug used in the treatment of various solid organ cancers, including cervical cancer. However, despite its effectiveness, oneof the limiting uses of CDDP is nephrotoxicity. AlthoughCDDP-induced nephrotoxicity is manifested in a number ofways, the most prominent outcome is acute kidney injury(AKI). Previous studies have been shown that approximatelyone-third of patients experience AKI after CDDP chemother-apy as evidenced by reduced glomerular filtration rate (GFR),increased blood urea nitrogen (BUN), increased serum creatinine (SCr), Cystatin C and NGAL. Cisplatin nephrotoxicity is associated with tubular epithelial cell toxicity; vasoconstriction in renal microvascular; and proinflammatory effects on the kidneys. Acute renal impairment (AKI/acute kidney injury) occurs in 20-30% of patients after the administration of cisplatin.3
Serum creatinine as a marker of renal function is commonly done to date, but this biomarker known to be less sensitive. First, creatinine cannot show rapid changes in renal function, eg in patients in unstable condition, but the other will increase in patients with less muscle mass/protein intake. Moreover, creatinine is not cleaned exclusively by glomerular filtration, but partly cleared by renal tubules. This phenomenon can result in under/overestimation of kidney function, especially kidney filtration rate.4 The new marker is now starting to be introduced is cystatin c and neutrophil gelatinase associated lipocalin (NGAL). Cystatin C is a substance produced by the body cells constantly, freely filtered through the glomerulus, reabsorbed and catabolized by proximal tubules. At the proximal tubular damage Cys C is not reabsorbed, so that high levels in blood and urine will be a marker of renal impairment. This substance is not affected by food, age, muscle mass and body surface area, so it is quite ideal to expect it to become a new alternative as a marker of renal function tests.5 Neutrophil gelatinase-associated lipocalin (NGAL) is a 25 kDa protein that can be used as an early biomarker of AKI. Serum NGAL and cystatin C may act as early markers of contrast-induced AKI in patients undergoing percutaneous coronary intervention compared creatinine.6 Other study evaluated changes of urinary biomarkers were compared at 4 hours, 8 hours, and 12 hours, and 1 day, 2 days, 3 days, and 4 days after cisplatin intravenous infusions (75 mg/m2) versus the baseline. There was a significan increase in urinary NGAL levels from 12 hours to 4 days (p < 0.05) compared to baseline after cisplatin infusion.7 Increased NGAL in human blood will occur when cells are under stress, such as infection, inflammation and neoplasma. On the condition of renal tubular damage, increased NGAL levels will then induce tubular re-epithelialization.8 There are some limitations in trying to compare sensitive biomarkers for CDDP-induced nephrotoxicity comparing creatinine, Cystatin C and NGAL after cisplatin induced espicially in patients with cervical cancer IIB.
This study will assess serum creatinine, serum cystatin C and Urinary Neutrophil Gelatinase Associated lipocalin (NGAL) as urine biochemical parameter to detect kidney abnormalities before and after cisplatin administration in patients with IIB cervical cancer who received neoadjuvant cisplatin. In this study we explored the potential of a cystatin c and NGAL as a new screening indicator of impaired kidney function compared to serum creatinine which has been commonly applied.
METHODS
This was an observational analytic study paired with time series design, conducted to patients with IIB cervical cancer according to FIGO-based criteria. Examination included serum creatinine, serum cystatin C and urine NGAL before and after the administration of cisplatin 1 to 4th in a dose of 50 mg/m2/week.
Inclusion criteria for the study were as follows: new patients with IIB cervical cancer who admitted to Oncogynecologic Integrated Outpatient Clinic with biopsy results of squamous cell ca, patients with normal BMI (18.5 to 29.9) and willing to join the study. Exclusion criteria included: patients with renal disease, refused to join the study, had a history of chemotherapy/radiotherapy before, pregnant and was suffering from an infection.
This is an obervasional study in pairs with time series. Data were collected from March to May 2015 and then analyzed using t test and Wilcoxon test. From sample size formula, we collected 14 patients with cervical cancer IIB who were indicated for cisplatin based chemotherapy. Research carried in gyenecologic ward while patients get chemotheraphy and material sample was processed at Prodia Laboratories Surabaya and Jakarta.
Statistical analyses were performed using the SPSS version 20.0 for Windows, analyzed with level of significance ≤ 0,05.
Conduct feasibility was obtained from the Ethics Committee for Basic Science Research/Clinics in Dr. Soetomo Hospital/Faculty of Medicine, University of Airlangga no. 252/Panke.KKE/IV/2015.
RESULTS
From all patients, the average age was 45.85 with the youngest 33 and the oldest 59 years. Based on the age at marriage, the average age was 16.36 years with an age range 13-20 years.
This study was conducted in patients with anatomic-pathology results of squamous cell carcinoma (SCC). From these, 35.7% were invasive keratinizing SCC and 64.3% non-invasive keratinizing SCC. During the study, one patient dropped out because refusing to continue treatment and chosing alternative treatments. Total cisplatin given to 14 patients was averagely 296.97 mg.
Table 1. Characteristics of sample
| N (%) | Min | Max | Mean | SD | |
| Umur Pasien | 14 | 33 | 59 | 45.85 | 7.86 |
| Usia Saat Menikah | 14 | 13 | 20 | 16.36 | 2.02 |
| Invasive Keratinizing SCC | 5 (35.7) | ||||
| Invasive Non Keratinizing SCC | 9 (64.3) |
After giving NAC Cisplatin for 4 times, the 14 patients were evaluated for their operability through deep (vaginal) examination and or through pelvic MRI. From 14 samples, only one (7.14%) was declared as operable for BSO radical hysterectomy and pelvic lymphadenectomy. A total of 13 other patients continued chemotherapy with paclitaxel to carboplatin 3 times. Their operability was subsequently re-evaluated after the last chemotherapy.
Kidney Parameters Before and After NAC Cisplatin
All samples were treated equally in terms of the provision of good hydration before and after chemotherapy and sampling was performed 12 hours after chemotherapy ended.
Serum Creatinine
The obtained data had normal distribution, so that further data were analyzed using paired t-test. Statistically significant difference (p <0.05) was found in serum creatinine in each group after 2nd and 4th cisplatin (Table 1).
Table 2. Serum creatinine before and after NAC cisplatin
| Mean (s.d) | Difference (s.d) | CI 95% | p | |
| SCr before cisplatin | 0.71(0.11) | |||
| Scr after cisplatin 1 | 0.71 (0.89) | 0.004 (0.83) | 0.04-0.05 | 0.849 |
| Scr after cisplatin 2 | 0.86 (0.21) | 0.15 (0.21) | 0.02-0.27 | 0.020* |
| Scr after cisplatin 3 | 0.76 (0.11) | 0.05 (0.12) | 0.02-0.12 | 0.127 |
| Scr after cisplatin 4 | 0.79 (0.12) | 0.09 (0.14) | 0.01-0.17 | 0.032* |
Serum Cystatin c
Cystatin c data after first cisplatin had normal distribution, so that further data were analyzed using paired t-test. However, cystatin c after 2nd until 4th cisplatin had no normal data, so we analyzed using Wilcoxon test. Cystatin C rose after 2nd cisplatin, but statistical significance (p <0.05) was only found after 4th ciplatin (Table 2).
Tabel 3. Cystatin c serum before and after NAC Cisplatin
| Mean (s.d) | Difference (s.d) | CI 95% | p | |
| SC before cisplatin | 0.69 (0.09) | |||
| SC after cisplatin 1 | 0.67 (0.12) | 0.02 (0.07) | 0.02-0.06 | 0.273 |
| SC after cisplatin 2 | 0.76 (0.17) | 0.06 (0.15) | 0.02-0.15 | 0.151 |
| SC after cisplatin 3 | 0.75 (0.17) | 0.06 (0.14) | 0.02-0.14 | 0.186 |
| SC after cisplatin 4 | 0.78 (0.15) | 0.09 (0.11) | 0.02-0.15 | 0.003* |
Urinary NGAL
The data obtained were not normally distributed, so that the data were analyzed further using the Wilcoxon test. Urinary NGAL was found to increase after cisplatin 1, but it was not statistically significant and then it declined slowly (Table 3).
Table 4. NGAL urine before and after NAC Cisplatin
| Median (Minimum-Maximum) | p | |
| NGAL before cisplatin | 41.79 (22-734.02) | |
| NGAL after cisplatin 1 | 40.84 (47-3656.13) | 0.363 |
| NGAL after cisplatin 2 | 22.39 (4.61-287.33) | 0.433 |
| NGAL after cisplatin 3 | 34.49 (4.61-184.61) | 0.594 |
| NGAL after cisplatin 4 | 27.19 (4.44-195.22) | 0.510 |
Based on the data, the difference of the three parameters (serum creatinine, serum cystatin c and urinary NGAL) during the four-times administration of the chemotherapy neoadjuvant cisplatin can be described. Serum creatinine and serum cystatin c reaches a maximum value after cisplatin 2nd and 4th, whereas urinary NGAL increased maximum starting after the first cisplatin (Figure 1).
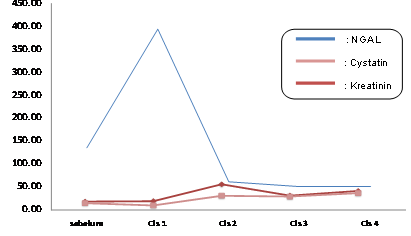
Figure 1. Differences in serum creatinine, serum cystatin c and urinary NGAL before & after NAC Cisplatin
DISCUSSION
According to FIGO recommendation, primary treatment for stage IIB cervical cancer is chemoradiation. Because of the limitations of radiation facilities in Indonesia in general and in Surabaya in particular, stage IIB cervical cancer in Surabaya is managed with treatment different from that of FIGO recommendation, that is the platinum-based neoajuvant chemotherapy followed with radical hysterectomy as long as the operability is possible.
A total of 14 IIB cervical cancer patients met the criteria as subjects in this study. The mean age of these patients was 45.85 years. Cervical cancer is known as a cancer of reproductive age. However, this cancer is also found in five, six and seven decades of life. The high incidence of cervical cancer in 4-5 decades in the present study samples reflects the lack of public awareness for the initial screening before cervical cancer has developed. The average age of patients with cervical cancer in the world is 51.4 years and there is a trend of increasing risk along with increasing age of the patients.9 In the USA, the average age of cervical cancer patients is around 52 years. Generally, women in higher ages do not have screened for cervical cancer. As a result, the incidence of the cancer in the population is higher than expected.10
The research data showed there were 14 patients with IIB cervical cancer with an average age range of was 16 years old when they got married. According Nesrin et al (2011) high risk of developing cervical cancer in those aged under 20 years old at the time of first sexual intercourse increased 4-5 fold compared to those with first sexual intercourse over the age of 20 years. This is because they are at the transition period from childhood towards adulthood, when an increase in the hormone estrogen causes vaginal wall cells become thicker. By beneficial bacteria, glycogen is also converted into vaginal acid. Vaginal atmosphere becomes acidic, so that the surrounding epithelial tissue changes into layers. When in such full of change situation sperm goes in, the change will be augmented. If there are injuries due to friction, epithelial cells will be disrupted and become abnormal.11
Sample used in this study was IIB cervical cancer of squamous cell carcinoma. This cell type was taken because almost 85% of cervical cancer cases are of squamous type and for the purpose of sample homogeneity. From epidemiological studies, squamous cell carcinoma of the cervix is closely linked to sexual behavior, such as sexual partner more than one, having high risk partners and early age at the first time of sexual intercourse.8 A total of 5 patients (35.7%) had invasive keratinizing SCC and 9 patients (64.3%) had invasive non-keratinizing SCC. Squamous cell carcinoma is the most common histopathological type in cervical cancer. There had been no prospective studies that discussed the management of specific cervical cancer based on its histopathological types.
Fourteen samples received cisplatin of 50 mg/m2/week for 4 times and then their operability was evaluated. Based on the data, the average total cisplatin given was 295.22 mg. Chemotherapy dose regulation at Dr. Soetomo Hospital is not related to patient’s age but rather to accompanying comorbidities, especially kidney and liver disease. There is no difference in dose between the elderly and younger patients. Dale (2003) states that there is no difference in the success of cancer treatment between older and younger patients when the same dose is given. LFG and plasma magnesium concentration decrease after cisplatin doses higher than 50 mg/m2 of body surface area, but it does not change if doses below 20 mg/m2 are given. All samples studied showed no significant toxic effects after cisplatin administration. Other patient-related variables increase the risk of nephrotoxicity; including female sex, older age, smoking, and hypoalbuminemia. In general, previous renal dysfunction increases the risk of AKI.3,12
After receiving neoadjuvant chemotherapy, the samples were evaluated for their operability. Evaluation carried out clinically through vaginal examination and confirmed by radiological examination (MRI), and thereafter declared as operable or inoperable. However, not all of the 14 patients did pelvic MRI examination because of long queues which could affect the progress of the disease. The tumor were evaluated after NAC in Gyneco-oncology Outpatient Clinic Dr. Soetomo Hospital. It was almost always done in the clinical course, since only a few patients had been evaluated with radiological examination (MRI). MRI is currently used as a tool to accurately determine tumor size and tumor size were obtained from measurements using MRI can be used as one predictive factor of recurrence and patients’ survival of. MRI can evaluate accurately the size of the tumor at the same time of tumors spread in cervical cancer, which cannot be measured appropriately by clinical method only.13
Patients who were regarded as operable were prepared to have radical hysterectomy, while patients regarded as non-operable could not be managed with operative measures. In this study, only 1 (7.14%) of 14 patients were declared operable and would do a radical hysterectomy surgery. Thirteen other patients were given with additional NAC in the form of carbo pacli 3x. Their operability would then be re-evaluated. As described previously, the treatment for IIB cervical cancer should be chemoradiation, but because of the limitations of radiotherapy in Dr. Soetomo Hospital, where the patients should wait for 6-10 months, neoajuvant chemotherapy is still be allowed provided the patient has been enrolled in radiotherapy since their first visit to Oncology Outpatient Clinic at Dr. Soetomo Hospital.
Research of Friyadi and Askandar (2013) examined the operability of 305 cervical cancer patients who received NAC in 2011-2013. From 130 patients who received cisplatin neoajuvant chemotherapy, as many as 20 patients were declared operable and all of them continued their treatment with radical surgery.14
Kidney parameters NAC after cisplatin exposure
More than 50 percent of cisplatin will be excreted in the urine in the first 24 hours after administration of cisplatin and platinum concentrations achieved in the renal cortex are several times larger than the accumulation of plasma and other organs. Cisplatin is primarily induced and hurt the S3 segment of proximal tubules, causing a decrease in glomerular filtration rate.15
Serum creatinine
Until then, the determination used for the diagnosis of AKI is based on serum creatinine, even in Dr. Soetomo Hospital. Creatinine is a compound formed from keratin and keratin phosphate derived from muscle. Creatinine is subjected to filtration in glomerulus and secretion in the tubule, then secreted into the urine.16
This study showed significant increase (p <0.05) in serum creatinine after 2nd and 4th of ciplatin (Table 1). However, no clinically significant differences were found in all sessions of serum creatinine examination (creatinine levels were still within normal limits).
There is a weakness of creatinine as a marker of kidney damage since the level is influenced by the amount of muscle mass that affects kreatinin secretion in the tubule and its reabsorbtion, protein intake, age and gender. In addition, sometimes blood creatinine increase ony after kidney function has been damaged of more than 50%, or, vice versa, creatinine in blood is still low even though the kidney has been damaged (creatinine blind zone).17 Therefore, in its interpretation creatinine often yields false positive or false negatives due to various factors above. To determine kidney damage or injury, therefore, creatinine examination should be followed by more kidney examinations to obtain better accuracy.18 Several studies have reported an increase in serum creatinine even in the absence of histopathological kidney damage, mainly in old age patients (reduced muscle mass) or those with less protein intake.19,24,26
Serum cystatin c
Cystatin c is an alternatative GFR marker because it has several advantages, including: protein with a molecular weight of 13kDa light, alkaline to high isoelectric point (pl) of 9.1 makes this protein free filtered and relatively stable; cystatin c undergoes perfect catabolism in tubules, with the result that its presence in circulating blood and in urine only in very small quantities, is not influenced by gender and time of samplling can be done any time.4
Although cystatin C appears to increase after 2nd cisplatin, but significant difference was found in cystatin c only after exposure to 4th of cisplatin in14 samples (Table 2). This phenomenon is different from that of Christensson et al., 2004 who examined 41 patients with type 1 diabetes and 82 patients with type 2. They found that cystatin c was significantly better to detect early-stage nephropathy (GFR <80ml/min/1.73m²) compared to serum creatinine.20 If related to GFR marker as gold standard in kidney damage, research by Benohr P, et al (2006) concluded that cystatin c is detected more sensitive to GFR inulin rather than creatinine post cisplatin administration, although the creatinine is increasing.21 Research from Hojs, et al., found that GFR from cystatin c marker better than creatinine in patients who have mild to moderate kidney disease (stage 2-3 CKD, GFR 30-89/ml/min/1.73m².22
In this study, we found no clinically significant difference in all-time examination of serum cystatin C (the value of cystatin C was in the normal range) (Table 2). It is probable that the difference was because the samples were patients with healthy kidneys, so that the kidney damage due to cisplatin tended to be reversible with a dose of 50 mg/m2 (non-toxic dose).
Urinary NGAL
NGAL is also called lipocalin-2, siderocalin, a protease resistant polypeptide. It is released from the distal tubule, with urine secretion ,or released into the plasma. NGAL expression, which is induced by injured epithelium, is the earliest components expressed by the kidney after ischemic injury in nephrotoxic test of the experimental animals.21
Based on the data, NGAL increased first than other parameters, precisely since cisplatin 1, but there was no significant differences in any cisplatin administration along the observation. Hsien Lin-HY et al. (2013) studied urinary NGAL, urine cystatin c, and urine albumin-creatinine ratio. They were examined on 4, 8, 12 hours, day 1 to 4 post-exposure to cisplatin 75 mg/m2 in 34 patients with head and neck cancer. The results showed that NGAL significantly increased in AKI group since the first 12-hour exposure to cisplatin even after adequate hydration, but not significant in all the time in non-AKI group. Urine NGAL proved was the first to increase compared to urine cystatin c and urine albumin both AKI and non-AKI groups. Urine NGAL increased 12 hours after cisplatin (p = 0.01), so it can be used as the predictor of AKI.7 NGAL seems to have specific increase in patients with AKI.
NGAL sensitivity and specificity could not be measured in this study because of minimal sample size. A study by Lawang SA, et al (2014) regarding urinary NGAL compared in patients with AKI and non-AKI obtained a sensitivity of 100%, specificity 63%, positive predictive value 27.27%, and negative predictive value of 100%. A sensitivity of 100% means the possibility of a diagnostic test result will be positive if done on a group of subjects who are sick. A specificity of 63% means that there is a 63% chance of diagnostic test results will be negative when performed on healthy subjects. Samples of this study were those who did not have a history of renal disease (healthy subjects). Negative predictive value of 100% is the possibility of urinary NGAL test stating that someone is absolutely not suffering from AKI. Meanwhile, the positive predictive value of 27.7% is the proportion of urine NGAL test possibility stating that a person is actually suffering from AKI. This means that urine NGAL has a very high sensitivity, while its specificity is not too high. In addition, its accuracy to declare a person not suffering from AKI is very high, with negative predictive value of 100%.23
Based on Figure 1, it appears that there was a rise in NGAL after the first exposure to cisplatin, whereas serum creatinine and serum cystatin c had only increased and reached the peak after cisplatin 2 and 4. This illustrates that NGAL increased first compared to other parameters. Padhy M. et al (2014), who observed renal function through creatinine, cystatin C and NGAL in patients undergoing coronary intervention using a contrast agent that can induce AKI, found that NGAL reached maximum levels in 4-hour examination (sensitivity 100%, specificity 96, 7%) and then it would be close to normal after 48 hours of exposure. Cystatin c reached maximum levels in the first 24 hours (sensitivity 100%, specificity 96.7%), while the new creatinine increase reaches the highest value after 48 hours.6
It is known that cystatin c and NGAL is a new parameter that can detect kidney damage earlier than creatinine. Hsien Lin HY et al (2013) compared the parameters of urinary NGAL, urinary cystatin and urinary albumin, evaluated on hour-4,8,12, day 1, to day 5 after exposure to cisplatin 75 mg/m2 in patients with cancers of the head and neck, oesophageal cancer and cancer of the thymus. They found that in AKI group, NGAL increased significantly (p <0.05) since the first 12 hours of exposure to cisplatin and cystatin c levels. Despite the increase obtained, statistically there was no difference in all observations. However, there were no significant differences in all parameters obtained before and after cisplatin in every observation in patients with non-AKI. This confirms the notion tha, in a healthy kidney injury caused by cisplatin is reversible.7
Normally, kidneys induced by toxic agent cisplatin will experience re-epithelization since the first day post-exposure, reaching a peak on day 5 to 7 and interstitial fibrosis was apparent in the lesion area on day 9 onwards. There is a positive correlation between immunohistochemical expression of NGAL and PCNA (proliferating cell nuclear antigen) that shows the regeneration of renal epithelial cells as a result of NGAL in cisplatin-induced mouse models.24
As a siderophor iron complex, NGAL serves to limit tubular damage and reduces apoptosis. This is explained by the ability of NGAL molecular binding agent that works for cellular transcription, including NF-kB. NF-kB is activated rapidly in renal tubular cells after acute injury and induces cell proliferation.8
The three parameters indicate that the 14 patients have not experienced serious renal impairment. This is because the study samples were patients with normal renal function. In addition, it could also be influenced by the dose of cisplatin, which was in the safe category (<50 mg/m2), and the provision of optimal hydration before and after chemotherapy. The risk of nephrotoxicity is increasing with dose, frequency of administration, cumulative dose of cisplatin and high concentration of free-plasma platinum peak. In addition, because cisplatin is excreted in the urine (35% -50% and disappeared after day 5) through renal tubular secretion and glomerular filtration in healthy kidney, cisplatin induction in the kidney was spontaneously resolved.25
The administration of intravenous saline solution will induce, which will significantly reduce the risk of nephrotoxicity. In nephrotoxic trial studies where intravenous saline solution was used for post-cisplatin hydration, more than 50% of the cases had significant decrease in the incidence of nephrotoxicity to a very low level. This allows cisplatin for clinical use continuously.15
Gynaecological Oncology Department at Dr. Soetomo Hospital used a regimen of cisplatin 50 mg/m2 for IIB cervical cancer therapy followed by the administration of hydration before and after chemotherapy, in the form of a solution consisting of 1000 ml of isotonic saline plus 20 mEq of potassium chloride and 1 gram of magnesium sulfate. Intravenous solution is given at least 1000 mL for 2-3 hours before cisplatin, and a minimally of 500 mL for two hours after cisplatin administration. This fluid should be sufficient to form urine at least 100 mL/hour for two hours before and two hours after chemotherapy administration.
Clinically, we did not find differences in serum creatinine, serum cystatin c and urinary NGAL before and after cisplatin chemotherapy in IIB cervical cancer patients. So it can be concluded that NAC cisplatin at a dose of 50 mg/m2/week can be safely administered to patients with IIB cervical cancer.
The limited number of patients classified for our research might be the reason there is no significant result between each parameter in the early stage of AKI after cisplatin induced. Further studies with large sample and then determining cut off level of NGAL and Cystatin C as a new biomarker following cisplatin treatment would help in developing strategies to make a focused approach to minimize cisplatin-associated nephrotoxicity, without reducing or interfering with its antitumor effects.
CONCLUSION
There is an increase of serum creatinine, serum cystatin c and urinary NGAL after cisplatin administration. Urinary NGAL increases first, so we assume that NGAL is a useful biomarker of AKI early detection after cisplatin treatment in IIB cervical cancer patients.
REFERENCES
- Depkes. Hilangkan Mitos Tentang Kanker. 2014 : http://www.depkes.go.id/article/print/201407070001/hilangkan-mitos-tentang-kanker.html. (accessed 23 Jan 2015).
- Divisi Onkoginekologi. Data kanker serviks di RSU Dr. Soetomo tahun 2010-2014. 2015. RSU Dr. Soetomo-Surabaya.
- Miller PR, Tadagavardi RK. Review: Mechanism of cisplatin nephrotoxicity. Toxins 2010;2:2490-518.
- Delanaye P, Cavalier E. Detection of decreased glomerular filtration rate in intensive care units : serum cystatin C versus creatinine. BMC Nephrology 2014:15-9.
- Vivien SS, Delayane P. Review: Cystatin C: Current position and future prospects. Clin Chem Lab Med 2008;46:1664–686.
- Padhy M, Khausik S, Girish MP, Mohapatra S, Shah S, Koner BC. Serum neutrophil gelatinase associated lipocalin (NGAL) and cystatin C as early predictors of contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention. 2014. http://dx.doi.org/10.1016/j.cca.2014.04.016. (accessed 27 Jan 2015).
- Hsien Lin-HY, Lee-SC, Lin SF, Hwang DY, Yang WC. Urinary NGAL levels predict cispltain-induced cute kidney injury better than albuminueria or urinary cystatin c levels. Kaohsiung Journal of Medical Sciences. 2013;29: 304-11.
- Chakraborty S, Kaur S, Guha S, Batra SK. The multifaceted roles of neutrophil gelatinase associated lipocalin (NGAL) in inflammation and cancer. Biochimica et Biophysica Acta 2014;1826: 129–69.
- Berek JS. Berek’s & Novak’s Gynecoogy, 14th ed. Philadelphia: Lippincott Williams and Wilkins; 2007. p. 129-47.
- Carmen M, Schorge J. Invasive cervical adenocarcinoma. 2014. :http://www.uptodate.com/contents/overview-of-approach-to-cervical-cancer-survivors (accessed 20 Jan 2015).
- Nesrin R, Nezihe K, Dilek K. Risk factors for cervical cancer: Result from hospital-based case control study. International Journal of Hematology and Oncology. 2011;21:155-7.
- Dale DC. Poor prognosis in elderly patients with cancer: the role of bias and undertreatment. J Support Oncol. 2003;1:11-7.
- Duska RL. Overview of approach to cervical cancer survivors. 2014. http://www.uptodate.com/contents/overview-of-approach-to-cervical-cancer-survivors (accessed 20 Jan 2015).
- Friyadi MH, Askandar B. Perbandingan operabilitas setelah pemberian kemoterapi neoadjuvan cisplatin dan paclitaxel-carboplatin pada kanker serviks IIB di RSUD Dr. Soetomo. Divisi OnkoGinekologi RSU Dr. Soetomo-Surabaya; 2013.
- Portilla D, Safar AM, Shannon M, Penson RL. Cisplatin nephrotoxicity. 2013. http://www.uptodate.com/contents/ cisplatin-nephrotoxicity (accessed 23 Jan 2015).
- Inker LA., Perrone RD. Assessment of kidney function. 2014. http://www.uptodate.com/contents/assessment-of-kidney-function (acessed 23 Jan 2015).
- Ibrahim A, Elrehim A. Evaluation of some biochemical in relation to acute renal failure. Suez Canal Veterinary Medicine Journal 2011;15:193-4.
- Fergusson MA, Vaidya VS, Bonventre JV. Biomarkers of nephrotoxic acute kidney injury. Toxicology 2008;245: 182–93.
- Paragas N, Qiu A, Hollmen M, Nickolas TL, Devarajan P. NGAL-siderocalin in kidney disease. Biochimica et Biophysica Acta. 2014;1823:1451-8.
- Christensson AG, Grubb AO. Serum cystatin C advantageous compared with serum creatinine in the detection of mild but not severe diabetic nephropathy. Journal of Internal Medicine. 2004:256;, 510-18.
- Benohr P, Grenz A, Hartmann JT, Muller GA, Blaschke S. Cystatin C, a marker for assessment of the glomerular filtration rate in patients with cisplatin chemotherapy. Kidney Blood Press Res. 2006;29:32-5.
- Hojs S, Bevc S. Serum cystatin C-based equation compared to serum creatinine-based equations for estimation of glomerular filtration rate in patients with chronic kidney disease. Clinical Neph. 2008;70:10-17.
- Lawang SA, Pudjiadi A, Latif A. Neutrophil gelatinase associated lipocalin urin sebagai deteksi dini acute kidney injury. Sari Pediatri Journal. 2014;16:195-201.
- Kashiwagi E, Tonomura Y, Kondo C, Masuno K, Fujisawa K, Tsuchiya N. Involvement of NGAL and osteopontin in renal tubular regeneration and interstitial fibrosis after cisplatin-induced renal failure. Experimental and Toxicologic Pathology. 2014;66:301-11.
- Florea AM, Büsselberg D. Cisplatin as an anti-tumour drug: Cellular mechanisms of activity, drug resistance and induced side effects. Cancers. 2011;3:1351-71.
- Togashi Y., Sakaguchi Y., Miyamoto M., Miyamoto Y. Urinary cystatin C as a biomarker for acute kidney injury and its immunohistochemical localization in kidney in the CDDP-treated rats. Experimental and Toxicologic Pathology. 2012:64: 797–805.
Post Terkait
PENGGUNAAN PROPOELIX™ UNTUK MENINGKATKAN IMUNITAS TUBUH PADA SUBJEK PENELITIAN YANG SEHAT
pemberian ekstrak propolis terjadi perubahan bermakna terhadap peningkatan kondisi klinis menjadi lebih baik dan pengukuran CD4, CD8 dan Sel NK pada subjek penelitian setelah mengkonsumsi Propoelix selama 30 hari dimana…
SelengkapnyaPrinsip-Prinsip Hak Asasi Manusia Dalam Pelayanan Kesehatan Dan Perlindungan Hak Kesehatan Bagi Orang Dengan Gangguan Jiwa
Hak Asasai Manusia adalah hak yang melekat secara inheren pada semua orang sejak lahir. Hak atas layanan kesehatan adalah salah satu hak yang berasal dari hak asasi manusia. Prinsip-prinsip Hak…
SelengkapnyaPerbandingan Dua Tabung Sitrat Pada Pemeriksaan Faal Hemostasis
Pemeriksaan faal hemostasis (FH) memegang peranan penting dalam tatalaksana kelainan koagulasi. Hasil pemeriksaan FH dapat dipengaruhi oleh banyak faktor muali dari preanalitik, analitik, dan pos analitik, Fase preanalitik melibatkan persiapan…
SelengkapnyaHubungan Antara Sindroma Metabolik, Obesitas dan Analisis Faktor Risiko terhadap Kejadian Bromhidrosis
Pendahuluan: Bromhidrosis merupakan kombinasi dari hiperhidrosis dan osmidrosis. Hiperhidrosis adalah suatu kondisi produksi keringat berlebih yang berasal dari kelenjar ekrin, sedangkan osmidrosis ditandai secara khas dengan adanya bau mengganggu berasal…
SelengkapnyaDiagnostik Reference Level (DRL) pada Pemeriksaan Radiologi Torax Pediatri di RSUP Dr. Saiful Anwar Malang
Latar belakang: Pasien pediatri memiliki potensi resiko efek radiasi sinar-x yang lebih besar dibandingkan dengan pasien dewasa. UNSCEAR melaporkan ada 23 tipe kanker yang berbeda ditemukan pada pasien pediatri. Lebih…
Selengkapnya
Dari Redaksi
Kolom
Artikel
PENGGUNAAN PROPOELIX™ UNTUK MENINGKATKAN IMUNITAS TUBUH PADA SUBJEK PENELITIAN YANG SEHAT
10 Sep 2021 02:09 Artikel Penelitian
Prinsip-Prinsip Hak Asasi Manusia Dalam Pelayanan Kesehatan Dan Perlindungan Hak Kesehatan Bagi Orang Dengan Gangguan Jiwa
09 Jul 2020 16:27 Artikel Penelitian
Perbandingan Dua Tabung Sitrat Pada Pemeriksaan Faal Hemostasis
09 Jul 2020 16:18 Artikel Penelitian
Tata Laksana Koinfeksi HIV dan Hepatitis C : Fokus Pada Direct Acting Antiviral (DAA)
09 Jul 2020 15:57 Tinjauan Pustaka
Retensio Urine Post Partum
09 Jul 2020 13:41 Tinjauan Pustaka
Perbandingan Dua Tabung Sitrat Pada Pemeriksaan Faal Hemostasis
09 Jul 2020 16:18 Artikel Penelitian
PENGGUNAAN PROPOELIX™ UNTUK MENINGKATKAN IMUNITAS TUBUH PADA SUBJEK PENELITIAN YANG SEHAT
10 Sep 2021 02:09 Artikel Penelitian
Prinsip-Prinsip Hak Asasi Manusia Dalam Pelayanan Kesehatan Dan Perlindungan Hak Kesehatan Bagi Orang Dengan Gangguan Jiwa
09 Jul 2020 16:27 Artikel Penelitian
Kegiatan
FIK UI Rancang Strategi untuk Memutus Rantai Infeksi pada Anak Sekolah
10 Jul 2020 10:16 Kegiatan
Fakultas Farmasi Universitas Indonesia (FFUI) meresmikan Empat Ruang Pendukung Pendidikan Akademik
10 Jul 2020 10:06 Kegiatan
Fakultas Farmasi UI Resmikan Laboratorium dan Ruang Apotek Simulasi
10 Jul 2020 10:00 Kegiatan
Deteksi Dini Saraf Penciuman, Cegah Kerusakan Otak !
02 Sep 2019 09:43 Kegiatan


